Bicep tendon injuries are not just common; they are a lurking menace for athletes and fitness enthusiasts alike! Whether you’re swinging a tennis racket, diving into a pool, or lifting weights at the gym, the risk of a bicep tendon injury is ever-present. These injuries can range from mild inflammation to catastrophic ruptures, with bicep tendinopathy being a frequent and often misunderstood consequence. In this electrifying exploration, we will delve into the mechanisms behind these injuries, the shocking pathophysiology of bicep tendinopathy, and the most effective rehabilitation strategies that can turn your recovery into a triumphant comeback!
Anatomy and Biomechanics: The Biceps Unveiled
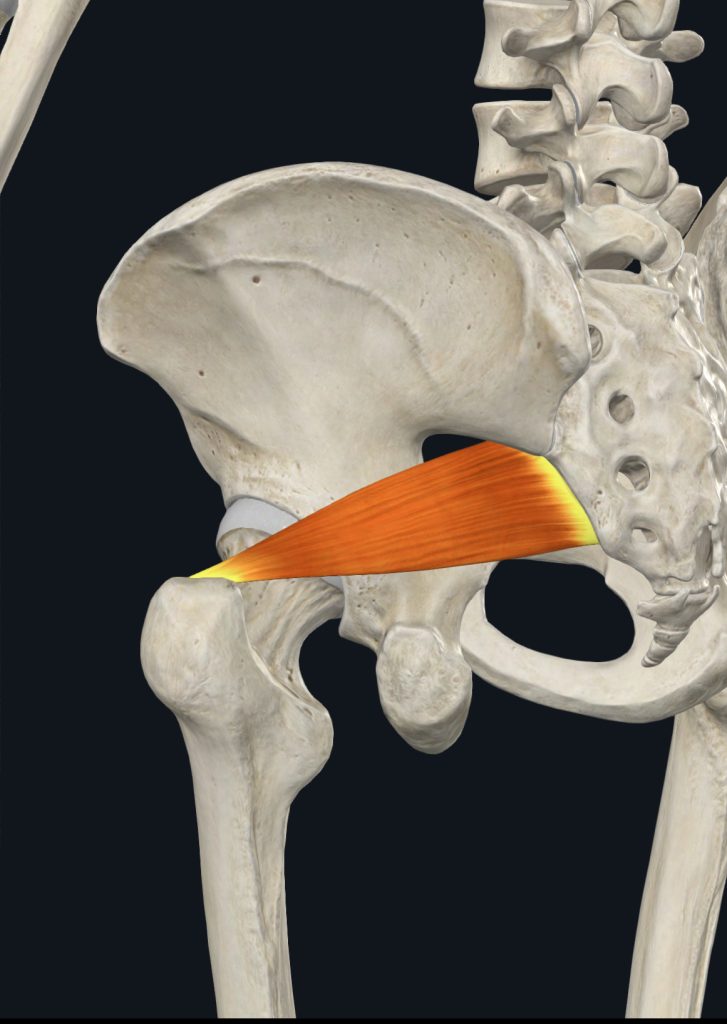
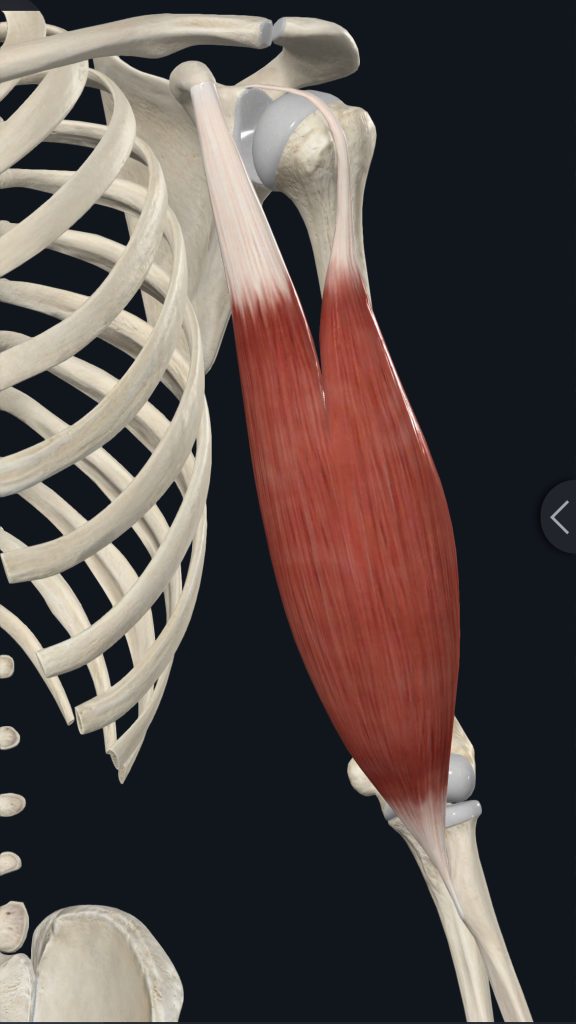
The biceps brachii muscle is a powerhouse with two heads: the long head and the short head. The long head springs from the supraglenoid tubercle of the scapula, traversing the bicipital groove of the humerus, while the short head originates from the coracoid process of the scapula. Together, they form a formidable tendon that inserts on the radial tuberosity of the radius. This muscle is not just for show; it’s the driving force behind elbow flexion, forearm supination, and even shoulder stabilisation!
Mechanisms of Injury: The Hidden Dangers
Bicep tendon injuries can strike when you least expect it, often due to:
- Repetitive Overhead Movements: Athletes in sports like swimming, tennis, and baseball pitching are particularly vulnerable.
- Heavy Lifting: Think bicep curls and chin-ups—these exercises can be a double-edged sword!
- Sudden Forceful Contractions: Imagine catching a heavy object or resisting a sudden elbow extension—ouch!
- Chronic Overuse: The slow burn of gradual degeneration can sneak up on you, leading to serious consequences.
These mechanisms can unleash a range of injuries, from tendinitis (acute inflammation) to tendinosis (chronic degeneration), partial tears, or even complete ruptures!
Whats actually going on here?
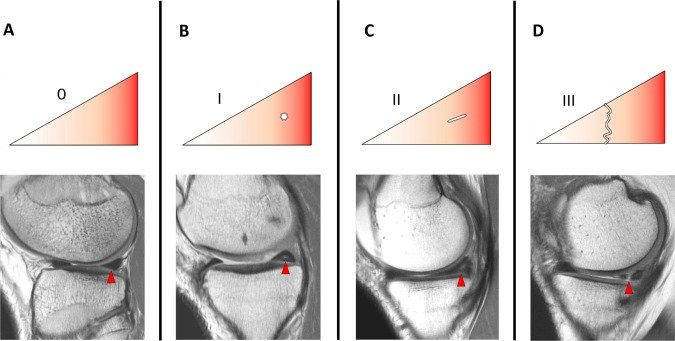
Bicep tendinopathy is a degenerative condition that transforms the tendon into a shadow of its former self. The process unfolds dramatically:
- 1. Initial Inflammation: Micro-tears in the tendon fibres trigger a fierce inflammatory response.
- 2. Failed Healing: Inadequate rest or continued stress prevents the tendon from healing properly.
- 3. Tendon Degeneration: Collagen fibres become disorganised, leading to a tendon that is thickened and less elastic.
- 4. Neovascularisation: New blood vessels form in typically avascular areas of the tendon, complicating matters.
- 5. Neural Ingrowth: New nerve endings develop, intensifying pain sensations.
The result? A tendon that is not only weakened but also more susceptible to further injury.
Rehabilitation Strategies: The Road to Recovery
Rehabilitating bicep tendinopathy requires a multifaceted approach that can lead to a triumphant return to activity:
Acute Phase (0-2 weeks):
- Rest and Activity Modification: Reduce stress on the tendon.
- Ice Therapy: Manage pain and inflammation effectively.
- Gentle Range of Motion Exercises: Prevent stiffness without overexerting.
- NSAIDs: Non-steroidal anti-inflammatory drugs can help manage pain. (Consult a doctor or pharmacist first)
Sub-Acute Phase (2-6 weeks):
- Progressive Loading Exercises:
- Isometric Exercises: Hold contractions without movement.
- Eccentric Exercises: Focus on the lengthening phase to build strength.
- Manual Therapy Techniques: Soft tissue and joint mobilisation can work wonders.
- Modalities: Ultrasound or low-level laser therapy can promote healing.
Remodelling Phase (6-12 weeks):
Progressive Resistance Training:
- Concentric and Eccentric Exercises: Target biceps and surrounding muscles.
- Plyometric Exercises: Boost power and function.
- Sport-Specific Training: Tailor exercises to your activity of choice.
- Return to Activity Phase (12+ weeks):
- Gradual Return to Full Activities: Ease back into your routine.
- Continued Strengthening and Flexibility Exercises: Maintain your gains.
Education on Proper Technique: Prevent future injuries with knowledge!
Key Principles of Effective Rehabilitation
- Progressive Loading: Gradually increase the load on the tendon to stimulate healing without overloading.
- Eccentric Focus: Eccentric exercises are particularly effective for tendinopathies, promoting collagen remodelling.
- Pain-Guided Approach: Exercises should only cause mild discomfort to avoid further irritation.
- Addressing Contributing Factors: Correct any biomechanical issues that may contribute to tendon stress.
- Patience and Consistency: Tendon healing is a slow process—commitment is key!
Advanced Rehabilitation Techniques: Pushing the Boundaries
- Blood Flow Restriction Training: This innovative technique allows for muscle and tendon adaptation with lower loads, reducing stress on the healing tendon.
- Instrument-Assisted Soft Tissue Mobilisation (IASTM): Specialised tools can enhance blood flow and promote healing.
Dry Needling: Inserting thin needles into trigger points can alleviate pain and improve function.
Conclusion: The Path to Triumph
Bicep tendon injuries, particularly bicep tendinopathy, demand a comprehensive and patient approach to rehabilitation. We can do this by embracing a structured program that respects the biological healing process, you can transform a potentially debilitating injury into a story of resilience and triumph. Here’s how you can ensure a successful recovery:
- 1. Commit to the Process: Understand that healing takes time. Stay dedicated to your rehabilitation program and trust the process.
- 2. Listen to Your Body: Pay attention to pain signals and adjust your activities accordingly. Pushing through pain can lead to setbacks.
- 3. Work with Professionals: Engage with an Osteopath, sports medicine specialists, and other healthcare providers who can tailor a program to your specific needs.
- 4. Stay Educated: Learn about proper techniques and body mechanics to prevent future injuries. Knowledge is a powerful tool in maintaining long-term health.
- 5. Stay Positive and Motivated: Mental resilience is as important as physical strength. Set realistic goals and celebrate small victories along the way.
Following these principles and embracing a holistic approach to recovery, you can not only overcome bicep tendon injuries but also emerge stronger and more knowledgeable. Remember, every setback is an opportunity for a comeback, and with the right mindset and strategy, you can achieve a full and triumphant return to your favourite activities.