I often get asked the question “when” in two very different ways from my patients, and I want to take a moment to chat about it. The first way comes from a place of acceptance. These are the folks who understand they have an injury and know that with the right information and a solid rehab plan, they’ll be back to their favourite activities in no time. It’s like they’re saying, “I get it, and I’m ready to do what it takes!”
Then there’s the second group, and I totally get where they’re coming from. These patients often ask “when” from a place of panic and despair. They might not have played competitive sports before, but they’re feeling the weight of not being able to join their beloved exercise classes. You can almost see the wheels turning as they negotiate with me about when they can return, creating a whirlwind of anxiety in the process. It’s not uncommon for the first part of our session to be about helping them calm down and find their center.
Now, you might think I lack empathy for these patients, but that couldn’t be further from the truth! Many of them attend these classes for deeply personal reasons, and mental health is often at the top of that list. I completely understand how the panic can set in when they feel like they’re missing out on something that brings them joy and stability.
But here’s the good news: I’m here to help all my patients become pain-free and get back to their chosen activities as soon as possible! Yes, like everyone else, I do have bills to pay, and the longer it takes to heal, the more I might earn. But honestly, that’s not my goal! The quicker you heal and feel great, the more likely you are to share your positive experience with others, and that’s what truly matters to me.
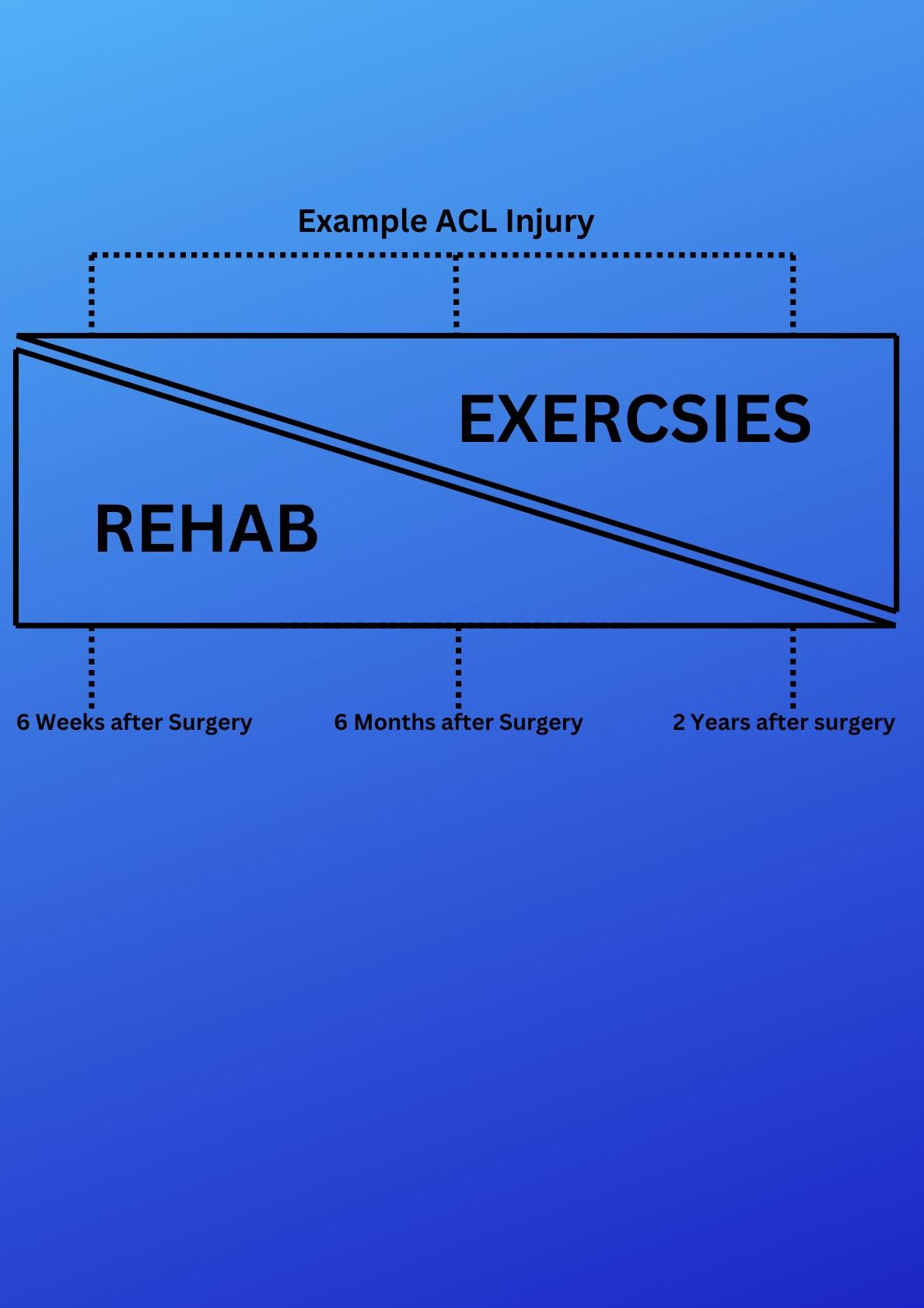
Rehab vs Exercise model
The diagram above illustrates a typical recovery timeline for an ACL injury over a two-year period. It’s important to note that the severity of an injury directly impacts healing time. For instance, while an ACL injury might take up to two years to fully recover, a less severe injury, like a muscle strain, could heal in as little as two months. In fact, many people can return to their workout classes just 2 to 4 weeks after a muscle strain!
The key takeaway here is: don’t despair! We’re all human, and the body has its own natural healing pace depending on the type of injury. While it can be frustrating, the best approach is to accept where you are in your recovery journey, focus on the right rehabilitation exercises, and work towards getting back to your favorite activities as soon as possible. Thanks for taking the time to read this!
Bicep tendon injuries are not just common; they are a lurking menace for athletes and fitness enthusiasts alike! Whether you’re swinging a tennis racket, diving into a pool, or lifting weights at the gym, the risk of a bicep tendon injury is ever-present. These injuries can range from mild inflammation to catastrophic ruptures, with bicep tendinopathy being a frequent and often misunderstood consequence. In this electrifying exploration, we will delve into the mechanisms behind these injuries, the shocking pathophysiology of bicep tendinopathy, and the most effective rehabilitation strategies that can turn your recovery into a triumphant comeback!
Anatomy and Biomechanics: The Biceps Unveiled
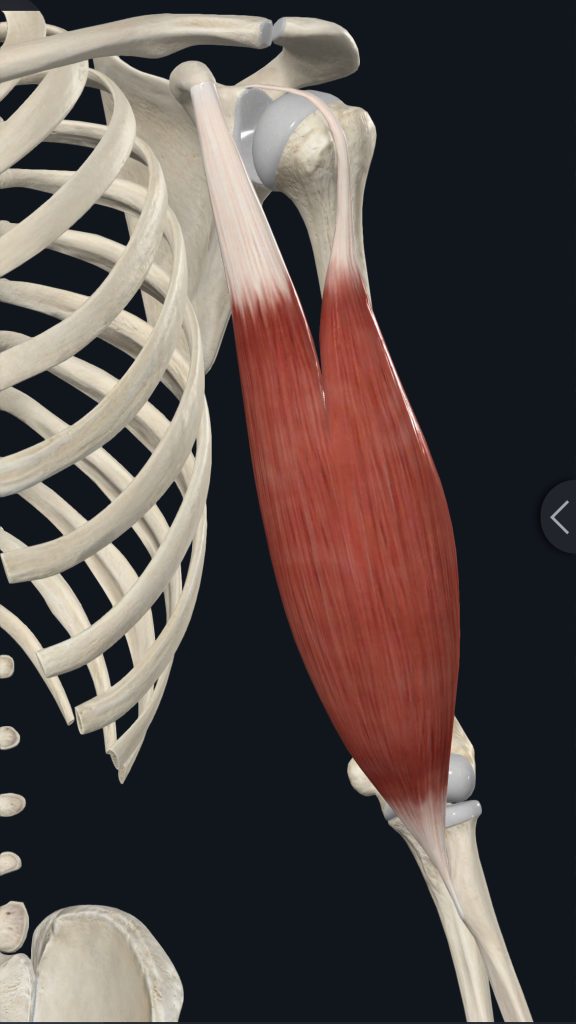
The biceps brachii muscle is a powerhouse with two heads: the long head and the short head. The long head springs from the supraglenoid tubercle of the scapula, traversing the bicipital groove of the humerus, while the short head originates from the coracoid process of the scapula. Together, they form a formidable tendon that inserts on the radial tuberosity of the radius. This muscle is not just for show; it’s the driving force behind elbow flexion, forearm supination, and even shoulder stabilisation!
Left Bicep Brachii
Mechanisms of Injury: The Hidden Dangers
Bicep tendon injuries can strike when you least expect it, often due to:
Repetitive Overhead Movements: Athletes in sports like swimming, tennis, and baseball pitching are particularly vulnerable.
Heavy Lifting: Think bicep curls and chin-ups—these exercises can be a double-edged sword!
Sudden Forceful Contractions: Imagine catching a heavy object or resisting a sudden elbow extension—ouch!
Chronic Overuse: The slow burn of gradual degeneration can sneak up on you, leading to serious consequences.
These mechanisms can unleash a range of injuries, from tendinitis (acute inflammation) to tendinosis (chronic degeneration), partial tears, or even complete ruptures!
Whats actually going on here?
Bicep tendinopathy is a degenerative condition that transforms the tendon into a shadow of its former self. The process unfolds dramatically:
1. Initial Inflammation: Micro-tears in the tendon fibres trigger a fierce inflammatory response.
2. Failed Healing: Inadequate rest or continued stress prevents the tendon from healing properly.
3. Tendon Degeneration: Collagen fibres become disorganised, leading to a tendon that is thickened and less elastic.
4. Neovascularisation: New blood vessels form in typically avascular areas of the tendon, complicating matters.
5. Neural Ingrowth: New nerve endings develop, intensifying pain sensations.
The result? A tendon that is not only weakened but also more susceptible to further injury.
Rehabilitation Strategies: The Road to Recovery
Rehabilitating bicep tendinopathy requires a multifaceted approach that can lead to a triumphant return to activity:
Acute Phase (0-2 weeks):
Rest and Activity Modification: Reduce stress on the tendon.
Ice Therapy: Manage pain and inflammation effectively.
Gentle Range of Motion Exercises: Prevent stiffness without overexerting.
NSAIDs: Non-steroidal anti-inflammatory drugs can help manage pain. (Consult a doctor or pharmacist first)
Sub-Acute Phase (2-6 weeks):
Progressive Loading Exercises:
Isometric Exercises: Hold contractions without movement.
Eccentric Exercises: Focus on the lengthening phase to build strength.
Manual Therapy Techniques: Soft tissue and joint mobilisation can work wonders.
Modalities: Ultrasound or low-level laser therapy can promote healing.
Remodelling Phase (6-12 weeks):
Progressive Resistance Training:
Concentric and Eccentric Exercises: Target biceps and surrounding muscles.
Plyometric Exercises: Boost power and function.
Sport-Specific Training: Tailor exercises to your activity of choice.
Return to Activity Phase (12+ weeks):
Gradual Return to Full Activities: Ease back into your routine.
Continued Strengthening and Flexibility Exercises: Maintain your gains.
Education on Proper Technique: Prevent future injuries with knowledge!
Key Principles of Effective Rehabilitation
Progressive Loading: Gradually increase the load on the tendon to stimulate healing without overloading.
Eccentric Focus: Eccentric exercises are particularly effective for tendinopathies, promoting collagen remodelling.
Pain-Guided Approach: Exercises should only cause mild discomfort to avoid further irritation.
Addressing Contributing Factors: Correct any biomechanical issues that may contribute to tendon stress.
Patience and Consistency: Tendon healing is a slow process—commitment is key!
Advanced Rehabilitation Techniques: Pushing the Boundaries
Blood Flow Restriction Training: This innovative technique allows for muscle and tendon adaptation with lower loads, reducing stress on the healing tendon.
Instrument-Assisted Soft Tissue Mobilisation (IASTM): Specialised tools can enhance blood flow and promote healing.
Dry Needling: Inserting thin needles into trigger points can alleviate pain and improve function.
Conclusion: The Path to Triumph
Bicep tendon injuries, particularly bicep tendinopathy, demand a comprehensive and patient approach to rehabilitation. We can do this by embracing a structured program that respects the biological healing process, you can transform a potentially debilitating injury into a story of resilience and triumph. Here’s how you can ensure a successful recovery:
1. Commit to the Process: Understand that healing takes time. Stay dedicated to your rehabilitation program and trust the process.
2. Listen to Your Body: Pay attention to pain signals and adjust your activities accordingly. Pushing through pain can lead to setbacks.
3. Work with Professionals: Engage with an Osteopath, sports medicine specialists, and other healthcare providers who can tailor a program to your specific needs.
4. Stay Educated: Learn about proper techniques and body mechanics to prevent future injuries. Knowledge is a powerful tool in maintaining long-term health.
5. Stay Positive and Motivated: Mental resilience is as important as physical strength. Set realistic goals and celebrate small victories along the way.
Following these principles and embracing a holistic approach to recovery, you can not only overcome bicep tendon injuries but also emerge stronger and more knowledgeable. Remember, every setback is an opportunity for a comeback, and with the right mindset and strategy, you can achieve a full and triumphant return to your favourite activities.
Piriformis syndrome is a neuromuscular disorder characterised by compression of the sciatic nerve by the piriformis muscle, resulting in pain and discomfort in the buttock and lower limb.
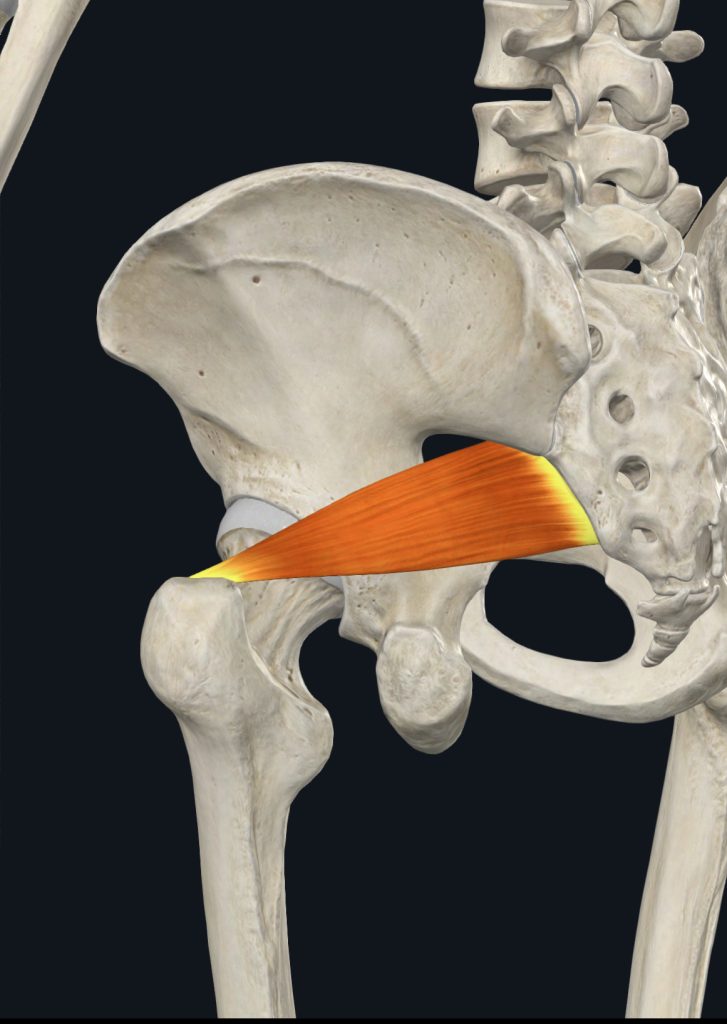
Anatomy
The piriformis is a flat, pear-shaped muscle located in the gluteal region. It originates from the anterior surface of the sacrum (S2-S4), passes through the greater sciatic notch, and inserts onto the superior aspect of the greater trochanter of the femur. The muscle functions as an external rotator of the hip when extended and an abductor when flexed.The sciatic nerve, the largest peripheral nerve in the body, typically passes beneath the piriformis muscle. However, anatomical variations exist where the nerve may pass through or above the muscle, potentially increasing the risk of compression.
Symptoms
Common symptoms of piriformis syndrome include:
Sharp, severe pain in the buttock
Radiating pain down the back of the thigh, calf, and foot
Numbness, tingling, or weakness in the affected leg
Discomfort with prolonged sitting or standing
Pain when walking up stairs or inclines
Muscle spasms in the piriformis region
Tenderness when pressure is applied to the muscle
These symptoms often worsen after prolonged sitting, walking, or running long distances. Pain may improve when lying on one’s back.
Pain Management and Rehabilitation
Several approaches can help manage pain and rehabilitate patients with piriformis syndrome:
Physical Therapy:
Stretching exercises targeting the piriformis and gluteal muscles
Strengthening exercises for the hip and core muscles
Manual therapy techniques like massage and myofascial release
Neuromuscular massage to release trigger points
Self-care Strategies:
Applying heat or ice to the affected area
Using a foam roller or tennis ball for self-massage
Taking frequent breaks from prolonged sitting
Modifying activities that exacerbate symptoms
Movement Re-education:
Improving posture and body mechanics
Learning proper techniques for daily activities and sports
Progressive Rehabilitation:
Gradually increasing activity levels as symptoms improve
Incorporating functional and sport-specific exercises
It’s important to note that treatment should be tailored to the individual, addressing the underlying cause of piriformis syndrome. A comprehensive approach combining various techniques often yields the best results in managing symptoms and preventing recurrence.
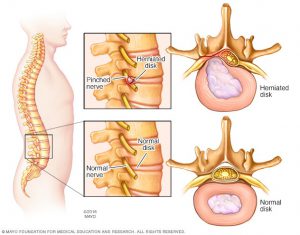
As many of you are aware, the disc does not slip as it is often thought of as a hockey puck. As the diagram shows, it is the gel like centre that protrudes out, which causes the discomfort as it irritates the nerve.
It is said that 80% of the worlds adult population have a disc bulge of sorts but are asymptomatic.
For those of you that have nerve pain as a result of a disc pathology then you have my up most sympathy, but even the symptoms differ from general morning stiffness to not being able to move.
A typical presentation of a disc pathology are usually to be stiffer in the morning (More than 1 hour) than during the day.
This is because the disc hydrates when we are sleeping and so there is more pressure placed on the bulge itself. When the disc shrinks through out the day, there is less pressure on the bulge. Equally, we are able to displace swelling when moving.
The Disc debate.
Often we see people that have been diagnosed, usually by an MRI, that they have a disc pathology. They have been told that the pain is from the disc pressing on a nerve.
In Clinic.
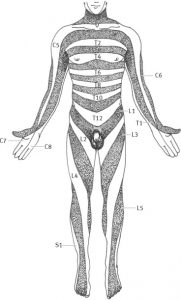
There have been many times where the person has had a disc issue, but the pain is not a direct result of that disc. For example, if you have an L5 disc herniation presenting with pins and needles or shooting pain in the front of your foot and shin, this is usual as this is where the sensory part of L5 goes to. See dermatome map.
Dermatome Map.
If you come to the clinic presenting with pain in the front of the thigh, having a disc issue at L5, the L5 disc maybe the overall cause, but its not directly causing the thigh pain. As you can see by the dermatome map.
Even if you have lower back pain, with no other symptoms and you happen to have an MRI showing you that you have a disc bulge, we cannot be completely sure that the disc is actually the problem.
Think of it this way, you only have test (mechanically speaking) when there are symptoms. For all we know you could have had that L5 disc bulge for a year or more.
What to do.
In any case, you have to keep moving and try to re-establish balance and movement in your body. The more you allow your body to become stiff, the more pain you will feel. There is no limit to the movement you should try, but always keep inside the remit of what you can do, as the body has a way of fighting back!