Meniscal injuries are a common type of knee injury that can vary significantly in severity, ranging from minor lesions to complex tears. The treatment approach, including the decision on whether surgery is necessary, depends on the grade, location, and type of meniscal tear. Here’s a detailed breakdown of the grading of meniscal injuries and their repairability:
Grading of Meniscal Injuries
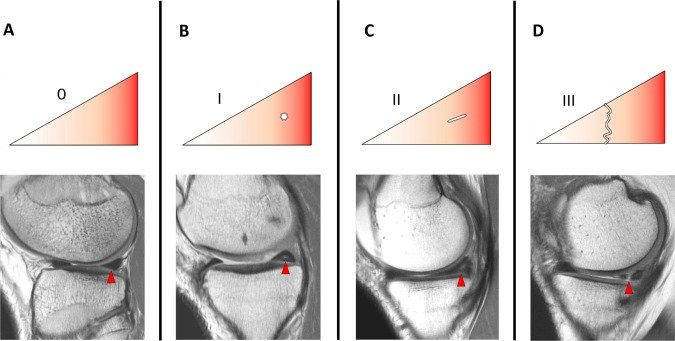
Meniscal injuries are classified into grades based on MRI findings, which help determine the severity and extent of the lesion:
Grade 1 (Mild Lesion)
Description: Small, punctate areas of hyperintensity within the meniscus that do not extend to the articular surface.
Repairability: Typically asymptomatic and do not require surgical intervention. These injuries are often treated conservatively with rest, physical therapy, and anti-inflammatory medications.
Grade 2 (Moderate Lesion)
Description: Linear areas of hyperintensity within the meniscus that still do not extend to the articular surface. Subcategories include:
Grade 2a: Linear signal without reaching the articular surface.
Grade 2b: Signal reaches the articular surface on a single MRI image.
Grade 2c: Wedge-shaped signal without reaching the articular surface.
Repairability: May still be managed conservatively if asymptomatic. If symptoms such as pain or swelling occur, physical therapy focusing on strengthening surrounding muscles is recommended.
Grade 3 (Definite Meniscal Tear)
Description: Hyperintensity extends to at least one articular surface (superior or inferior) on multiple consecutive MRI images, classified as a true meniscal tear.
Repairability: May require surgical intervention if symptoms persist or if there is mechanical instability (e.g., locking or catching of the knee). Surgical options include meniscal repair or partial meniscectomy, depending on the tear’s location and type.
Grade 4 (Complex Tear)
Description: Multiple disruptions in the meniscus with extensive damage to its structure, often involving both superior and inferior surfaces and may include displaced fragments.
Repairability: Often require surgery due to their severity. Repair is feasible if the tear is located in a vascularised region (the “red zone”). If repair is not possible, partial or total meniscectomy may be performed.
Factors Influencing Repairability
The decision to repair a meniscal tear depends on several factors:
Location of Tear
Red Zone: Outer third with good blood supply; tears in this zone have a higher likelihood of healing with repair.
Red-White Zone: Middle third with limited blood supply; repair success depends on individual factors.
White Zone: Inner third with no blood supply; tears in this zone typically cannot heal and are often treated with partial meniscectomy.
Type of Tear
Longitudinal tears near the red zone are more likely to be repaired successfully.
Complex or radial tears in avascular regions are less likely to heal and may require resection.
Patient Factors
Younger patients with healthy meniscal tissue have better outcomes after repair.
Older patients or those with degenerative changes may require alternative treatments.
Non-Surgical Management
For Grade 1 and Grade 2 injuries or stable tears that do not cause significant symptoms, non-surgical management is often effective:
Rest and Activity Modification: Avoid activities that exacerbate pain or stress the knee joint.
Physical Therapy: Strengthening exercises for quadriceps, hamstrings, and hip muscles to improve knee stability, and range-of-motion exercises to prevent stiffness.
Medications: Nonsteroidal anti-inflammatory drugs (NSAIDs) to reduce pain and swelling.
Bracing: Knee braces may provide additional support during recovery.
Surgical Intervention
Surgery is typically considered for Grade 3 and Grade 4 tears when conservative treatments fail or when there is mechanical instability:
Meniscal Repair: Indicated for longitudinal tears in vascularized zones (red zone). Success rates range from 85–90%, especially when combined with procedures like anterior cruciate ligament (ACL) reconstruction.
Partial Meniscectomy: Involves removing damaged portions of the meniscus while preserving as much healthy tissue as possible. Often performed for complex tears in avascular zones.
Total Meniscectomy: Rarely performed due to long-term risks of osteoarthritis. Reserved for cases where no other surgical options are viable.
Meniscal injuries range from mild lesions (Grade 1) to complex tears (Grade 4). While Grades 1 and 2 are typically managed conservatively without surgery, Grades 3 and 4 often require surgical intervention depending on factors such as tear location, type, and patient characteristics. Early diagnosis and appropriate treatment are crucial for preserving knee function and preventing long-term complications such as osteoarthritis.